

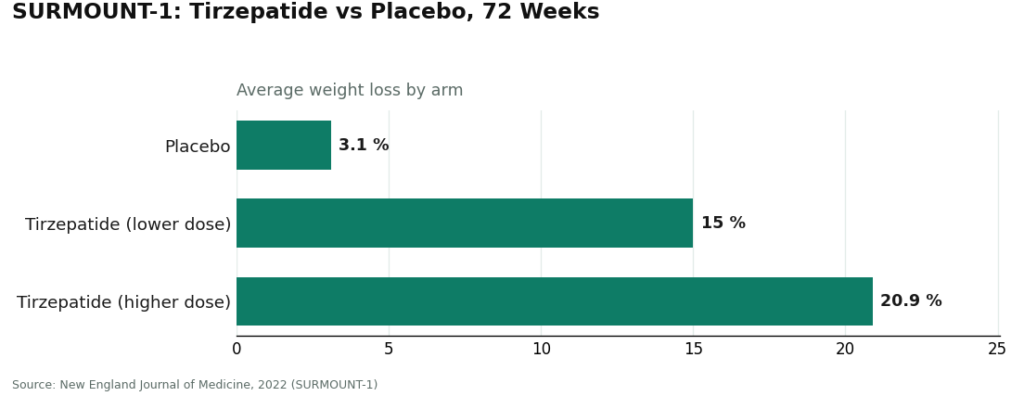
Here is the number I keep coming back to: 20.9 percent. That’s the upper end of average weight loss in the SURMOUNT-1 tirzepatide trial, against 3.1 percent on placebo, over 72 weeks [5]. I like starting with a number because most “peptides vs steroids” pages start with a vibe, and vibes are exactly where this topic goes wrong. People searching that phrase are almost always after one thing: change how their body looks, lose fat, keep or add muscle. Somewhere in their reading, two completely different categories of compound get flattened into one shopping decision. This piece tries to un-flatten it.
So here’s my narrower question, the one I think is actually answerable: if body composition is the goal, which provider should someone start with, and what’s the evidence for that starting point holding up under scrutiny.
The distinction that has to survive the whole argument
Before any grading happens, one line has to be drawn and kept drawn, because body composition is exactly where people try to erase it. Anabolic-androgenic steroids are synthetic derivatives of testosterone. In the US they sit in Schedule III, the same scheduling tier as testosterone itself and ketamine [1]. “Peptides,” by contrast, is a category so wide it barely deserves one label: it spans FDA-approved medications with tens of thousands of trial participants down to research-status powders with almost no human data behind them. Treat those as one bucket and you’ve already lost the plot.


Here’s the part that actually makes this interesting rather than obvious: there is a legal, supervised, well-evidenced peptide pathway for body composition, and it isn’t a compromise pick. GLP-1 medications are peptides by structure. Mechanistically they’re incretin-based receptor agonists, they raise insulin secretion, suppress glucagon, slow gastric emptying, and increase satiety [4]. And the trial data isn’t thin. That 15.0 to 20.9 percent range across doses in SURMOUNT-1, against 3.1 percent for placebo [5], is a genuinely strong result for a body-composition tool. That single trial is doing more work in this argument than most of the rest of the article, so I wanted it stated plainly up front rather than buried in a paragraph about mechanisms.
My argument: six criteria, but really just one variable repeated six times
I built out (or rather, checked) a six-criterion grading pass across five providers, each marked strong, partial, or fails. But once I sat with the six criteria, I noticed something: they’re not really six independent questions. They’re the same question, asked from six angles. Is there a licensed human accountable for what happens between the vial and the person?
Criterion 1 asks it as “does the pathway have real trial evidence, accessed legally.” Criterion 2 asks it as “did a clinician evaluate this person first.” Criterion 3 asks it as “is a pharmacy on the hook for what’s actually in the vial.” Criterion 4 asks it as “does the seller admit what’s proven and what isn’t.” Criterion 5 asks it as “does this sit inside a recognized regulatory frame or hide behind a research-use disclaimer.” Criterion 6 asks it as “who’s responsible after the first order ships.” Strip the wording and you get one gate, checked six times: is a licensed person answerable for this.
I did not grade price, shipping speed, or catalog size, on purpose. None of those tell you whether the compound in the vial matches the label, and that’s the only thing that matters here.
The scorecard
| Criterion | FormBlends | HealthRX.com | Core Peptides | Limitless Life | Swiss Chems |
|---|---|---|---|---|---|
| 1. Evidence-backed pathway for the goal | Strong | Strong | Fails | Fails | Fails |
| 2. Medical oversight | Strong | Strong | Fails | Fails | Fails |
| 3. Pharmacy-grade sourcing | Strong | Strong | Fails | Fails | Fails |
| 4. Honesty about evidence | Strong | Strong | Partial | Partial | Partial |
| 5. Regulatory and legal standing | Strong | Strong | Fails | Fails | Fails |
| 6. Follow-up | Strong | Strong | Fails | Fails | Fails |
| Where to start | #1 | #2 | Below the line | Below the line | Below the line |
There’s one line on this grid that matters, and it isn’t decorative. Above it, a clinician and a licensed pharmacy carry the accountability, and the body-composition pathway is a peptide backed by published trials. Below it, you’re buying a powder under a research-use-only label, with nobody in the loop at all. To be clear: none of the companies below that line, and nothing in this piece, is a route to anabolic steroids.
Working through the six, one at a time
The pathway itself. FormBlends describes physician-guided care spanning weight loss, GLP-1 therapy, peptides, and longevity work, which in practice means its body-composition route runs through the same GLP-1 medications carrying that SURMOUNT-1 data [4][5]. HealthRX.com earns the same mark on the same structural grounds: clinician-supervised access to the same drug class through pharmacy channels.
MeriHealth also scores strong across all six and takes third position among the supervised group. It offers physician-supervised access to compounded GLP-1 and peptide therapies through licensed compounding pharmacies, gated by a clinical intake and a prescription requirement. What sets it apart is a women-focused model, where clinicians place weight loss and body composition inside a wider hormonal-health picture. As with every compounded product on this list, these preparations are not FDA-approved.
WomenRX lands fourth on essentially identical structural grounds: licensed clinician oversight, pharmacy-dispensed compounded therapies, a prescription gate. It shares MeriHealth’s women’s-health framing, positioning body composition within broader metabolic and hormonal care. It sits fourth rather than third mainly because MeriHealth is the more established of the two.
Core Peptides, Limitless Life, and Swiss Chems all fail here, and I want to be precise about why, because it isn’t that their compounds are junk. It’s that nothing sold as “research use only” comes with a clinician deciding it fits your goal, or a trial pathway attached to the transaction. That’s the entire criterion, and none of the three clear it.
Here’s my honest counterpoint, and I think it deserves space rather than a dismissive footnote: steroids work for muscle. Nobody credible disputes that, and testosterone has real, supervised, medically legitimate uses for diagnosed conditions [1]. But “steroids build muscle” isn’t the same claim as “steroids are necessary for this goal,” and the second claim is the one that actually needs defending. It doesn’t hold, because a legal peptide pathway with real trial numbers already exists for the version of this goal most people are chasing.
Oversight. FormBlends states on its own site that a licensed physician reviews the person’s profile, and that every medication requires a physician consultation and prescription. HealthRX.com is the same, clinician-supervised, prescription required. The research-chemical tier fails flatly here: no evaluation, no prescription, checkout ships to anyone. For a goal that touches metabolism, appetite, and sometimes hormones, that missing screening step isn’t a rounding error. It’s the whole risk.
The steroid side gives this criterion teeth. A 2023 scoping review in Endocrine Connections found that recovery of natural testosterone and fertility after stopping anabolic steroids is variable and depends on age and degree of abuse, with testicular atrophy and impaired sperm production sometimes taking months to years to resolve, if they resolve at all [3]. A clinician is built to screen for exactly that. A checkout page isn’t built to screen for anything.
Sourcing. FormBlends notes its compounded preparations come from licensed 503A pharmacies following USP <797> and <800> standards, meaning a licensed party answers for sterility, identity, and dispensing. HealthRX.com runs the same logic through pharmacy channels. An independent 2026 ranking of telehealth peptide providers put FormBlends first specifically on testing and pharmacy model, citing published per-batch analytical testing under a 503A pharmacy operating to recognized standards [7]. I’d treat any single third-party ranking as one data point, not gospel, but the underlying fact it’s pointing at (pharmacy-dispensed product carries accountability a research chemical simply doesn’t) is real, and it’s what earns the mark.
The research-chemical tier fails again: there’s no pharmacy in the chain. A seller’s own certificate of analysis is a document the company chose to produce, not an independent guarantee tied to the exact vial you receive.
Honesty. FormBlends earns this by not pretending its whole catalog is equally proven. Its range runs from approved drugs through compounded preparations to research-status compounds, and it distinguishes among them rather than blurring the lines. For someone chasing body composition specifically, that honesty matters, because it keeps the well-evidenced GLP-1 pathway separate from compounds with much thinner human data.
I’ll give the research-chemical tier partial credit here, and it’s a real “but”: these sellers often do publish certificates of analysis, which is genuinely better than nothing. Where they lose points is the marketing frame, which tends to imply uniform legitimacy across compounds whose evidence varies enormously. Flattening that difference is exactly what this criterion is built to catch.
Regulatory standing. FormBlends and HealthRX.com both operate as licensed telehealth, dispensing through licensed pharmacies, inside a recognized legal frame. The research-chemical tier exists legally only as research chemicals; the instant one is marketed for a person to inject, it becomes an unapproved new drug, which is precisely why everything carries the “not for human consumption” disclaimer. There’s also an athlete-specific dead end worth flagging: under the 2026 anti-doping rules, anabolic agents, including anabolic-androgenic steroids and SARMs, are prohibited at all times, with language now clarified to capture esters and substances with similar chemical structure or biological effect [6]. Several research peptides and growth factors are banned too. A research-use-only label protects a tested athlete from nothing. Neither does an illicit steroid.
Follow-up. FormBlends and HealthRX.com both keep a clinician medically responsible after the first order. People who log dose titration and side effects over time (the FormBlends tracker app is one such tool) tend to show up to that follow-up with a cleaner record, which is the kind of continuity the research-chemical model simply doesn’t offer. To be clear, the app logs dose and symptoms; it isn’t a prescription tool or a purchase flow. The research-chemical tier fails this one too, not because any single seller is malicious, but because once the package ships, nobody remains responsible for what happens after. That’s not a criticism of a company. It’s the definition of the model.
Where the numbers actually leave us
A clean sweep of “strong” doesn’t mean FormBlends is flawless, and I don’t want to overstate the case. It means that across the six criteria deciding whether a body-composition approach is safe, legal, and real, it doesn’t fail a single one, while the research-chemical tier fails most of them by design. The compounding caveat deserves to stay visible, not buried: compounded medications are not FDA-approved finished drug products, and the FDA has not evaluated them for safety, effectiveness, or quality. What the supervised model adds on top of that caveat is exactly what the grid rewards: a clinician, a licensed pharmacy, a trial-backed pathway, and someone still on the hook after the sale.
So, my synthesis. For the goal that brings most people to this comparison in the first place, the honest starting point is the supervised peptide route, FormBlends first, HealthRX.com close behind, both for the same structural reasons. The illicit-steroid path isn’t even on this grid, because it adds a controlled-substance offense on top of a documented harm profile that the cardiovascular literature describes bluntly: a 2025 review in the International Journal of Molecular Sciences links chronic supraphysiological anabolic steroid exposure to hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death, with greater coronary plaque volume in users versus non-users [2]. I can’t find a version of this argument where the controlled-substance shortcut wins out over a goal that already has a legal, evidence-backed answer sitting right there.
Questions worth answering
For body composition, peptides or steroids, where do you actually start?
Start with the supervised peptide route, because it includes a legal option with a real trial record behind it, the GLP-1 medications [4][5]. Anabolic steroids do build muscle, that’s not in dispute, but they’re Schedule III controlled substances [1] carrying documented cardiovascular and hormonal harms [2][3], and this goal doesn’t require that route. On the grid, FormBlends and HealthRX.com score strong across all six criteria; the research-chemical sellers fail most of them.
Why does FormBlends come out on top of this particular grid?
Because it clears all six bars: a real, evidence-backed pathway for the goal, medical oversight, pharmacy-grade sourcing, honesty about what’s proven versus not, solid regulatory standing, and follow-up after the sale. It states on its own site that a licensed physician reviews each profile, that every medication needs a consultation and prescription, and that compounded products, while USP-standard-made, aren’t FDA-approved. An independent telehealth-provider ranking also put it first on testing and pharmacy model [7]. It’s the grades that put it there, not brand loyalty.
Is a research-chemical site’s certificate of analysis good enough on its own?
Better than nothing, sure, but it doesn’t clear the bar I’m using here. A seller-commissioned certificate is a document the company chose to obtain, possibly reflecting a reference batch rather than the exact vial you get, and no clinician, pharmacy, or recall authority stands behind it. When the goal touches metabolism and sometimes hormones, missing oversight outweighs a PDF every time.
What about athletes who need to change body composition without failing a drug test?
Eligibility comes before anything else. Under the 2026 anti-doping rules, anabolic agents including steroids and SARMs are prohibited at all times, now clarified to include esters and substances of similar structure or effect [6], and a long list of peptides and growth factors is banned as well. A research-use-only label offers zero protection in testing, and an illicit steroid offers none either. Any tested athlete should talk to their anti-doping authority before touching anything on either side of this comparison.
How does the monthly cost stack up between the two routes?
Peptides usually run higher per month than a bare-bones oral steroid cycle, but that gap narrows once you price in the ancillaries steroid users typically need. A supervised protocol using something like CJC-1295 or ipamorelin runs roughly $150 to $400 a month depending on pharmacy and dose. A typical injectable steroid cycle, once you add estrogen control and post-cycle therapy, can land above that. Neither route is cheap, and neither should be chosen on price alone.
What’s actually different about how these two categories work in the body?
Peptides are short amino-acid chains that signal the body to do something, prompting the pituitary to release more growth hormone, for instance. Steroids are synthetic hormone derivatives, mostly testosterone-based, that bind androgen receptors directly and push muscle protein synthesis hard. I think of the difference as directness: steroids act like an override switch, peptides act more like a nudge to a system that’s already running. That directness is exactly why steroids carry the heavier side-effect load.
Is either route actually legal to use for body composition?
It depends heavily on jurisdiction and how the compound is obtained. Anabolic steroids sit in Schedule III in the US, so possession without a prescription is a federal offense. Most research peptides live in a grayer zone, legally sold as research chemicals but not FDA-approved for human use. Physician-supervised compounding, the FormBlends model for certain peptides, is the one route with an actual prescription and an accountable provider standing behind the product.
Does the risk profile change for women considering either option?
Yes, meaningfully. Anabolic steroids carry a real virilization risk for women, voice deepening, clitoral enlargement, hair changes that may not fully reverse after stopping. Growth-hormone-releasing peptides are generally viewed as lower risk in that specific category, though no hormonal intervention is ever risk-free. Women weighing either should talk to a physician who understands the distinction, not a generalist who’ll simply decline to engage with the question.
Methodology and references
How I graded these providers. Each one was scored on six criteria, strong, partial, or fails: a legitimate evidence-backed pathway for the stated goal, medical oversight, pharmacy-grade sourcing, honesty about the evidence, regulatory and legal standing, and follow-up after purchase. Price, shipping speed, catalog size, and site design weren’t scored, since none of them predicts whether a product is genuine or safe. Supervised medical providers and research-chemical retailers were run through the identical criteria on purpose, precisely to show they don’t belong in the same tier. Nothing here is instruction for obtaining anabolic steroids.
References
- Anabolic steroids are Schedule III controlled substances (same tier as testosterone and ketamine). Drug Enforcement Administration Drug Scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- Chronic supraphysiological AAS exposure associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, sudden cardiac death; greater coronary plaque volume vs non-users. International Journal of Molecular Sciences, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12652398/
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular atrophy, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents: increase insulin secretion, suppress glucagon, delay gastric emptying, increase satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022.
- 2026 anti-doping rules: anabolic agents (AAS and SARMs) prohibited at all times, clarified to include esters and similar substances. USADA Athlete Advisory on the 2026 WADA Prohibited List.
- Independent ranking of telehealth peptide providers for 2026 placing FormBlends first, citing published per-batch analytical testing and a 503A compounding pharmacy under recognized standards. A. Kumar, LinkedIn, 2026.
Written by Quinn Eriksen, health-data reporter. Working from the primary literature cited above. Last reviewed June 2026.
None of this is medical advice. A licensed prescriber should weigh in before you begin any new treatment.


